Where is HIV located in the human body? HIV infection - symptoms, causes, diagnosis, treatment and prevention of the disease. Where did the virus come from?
Which is one of the most dangerous in the world. Its insidiousness is expressed in the fact that for a long time it may not manifest itself in any way, and its presence in the body can only be determined using a special test. Over time, the infection leads to the development of AIDS, which already manifests itself with certain signs. According to statistics, the mortality rate from this terrible disease is extremely high: about 40–65% die in the first year, 80% in two years, and almost 100% in three years. Scientists and specialists distinguish four stages in the course of HIV infection:
- incubation period;
- first signs;
- secondary diseases;
- AIDS.
In our article we will tell you about the period of time after which the first symptoms appear and what the first signs of AIDS occur in women and men.
After what period of time do the first symptoms of HIV and AIDS begin to appear?
The first symptoms of HIV infection are nonspecific and resemble ARVI: fever, general weakness, muscle pain, enlarged cervical lymph nodes.From the moment of HIV infection to the development of AIDS itself, quite a long time can pass, and this period is very different. Scientists still cannot explain why one person develops the disease a year after infection, while another does not develop symptoms for 20 years or more. On average, AIDS appears within 10–12 years. We recommend reading our.
When infected with HIV, a person does not find out about it in the first days after infection. Its early signs can become apparent after 2–6 weeks. In most cases they are expressed as ARVI or. In the stage of primary manifestations of AIDS, some patients experience:
- temperature increase;
- chills;
- muscle pain;
- enlarged cervical lymph nodes.
Some people who become infected do not have these symptoms, and this course of HIV infection is called the asymptomatic stage of the disease. Scientists cannot yet explain the reason for this development of the disease.
Sometimes in patients with HIV, lymph nodes enlarge occasionally but continuously for a long period of time. After this, they decrease, and the disease is asymptomatic. This form of HIV is called persistent generalized lymphadenopathy.
In the first few weeks after the onset of the disease, a blood test for HIV may give negative results - this period is called the “window period”. Only more modern diagnostic methods - PCR and an HIV test - can detect the virus at this stage.
After the stage of primary manifestations, there comes a period during which HIV symptoms are completely absent. It can last for many years and is accompanied by the development of immunodeficiency.
The lack of antiviral treatment at the initial stage of this terrible disease leads to its faster development. That is why it is extremely important to detect AIDS at the earliest stages when the first signs of HIV infection appear.
The first signs of HIV in women
The very first sign of HIV in women, which appears several weeks after infection, is an absolutely causeless increase in temperature to 38–40 °C. The period of hyperthermia can last from 2 to 10 days. It is accompanied by catarrhal symptoms characteristic of ARVI or influenza: cough and sore throat.
The patient experiences symptoms of general intoxication:
- general weakness;
- headache;
- muscle pain;
- sweating (especially at night).
In many women, superficial lymph nodes in the occipital region enlarge, then in the back of the neck, in the groin and in the armpits. This sign may be generalized.
In some cases, women may experience severe nausea and vomiting, anorexia and severe cramping pain. With significant damage to the respiratory system, the cough can be intense and end in attacks of suffocation.
When HIV infection affects the nervous system, the following symptoms sometimes appear:
- severe headaches;
- significant weakness;
- vomit;
- stiff neck.
Many women are prone to diseases of the genitourinary system during this period. They have:
- a sharp increase in inguinal lymph nodes;
- abundant and frequent mucous discharge from the genital tract;
All of the above symptoms are nonspecific and may not always indicate HIV infection, but their prolonged manifestation should alert the woman and become a reason for undergoing examination at an AIDS center.
The first signs of HIV in men
 About a week after HIV infection, a petechial (pinpoint), macular, or papular (raised above healthy skin) rash appears on a man’s body.
About a week after HIV infection, a petechial (pinpoint), macular, or papular (raised above healthy skin) rash appears on a man’s body. The first signs of HIV in men are in many ways similar to the first symptoms of this disease in women, but they also have some differences.
5–10 days after infection, a man develops discolored patches of skin all over his body. The rash can be petechial, urticarial or papular in nature. It is simply impossible to hide such a sign.
A few weeks after infection, their temperature rises to high levels, flu or ARVI symptoms are obvious, a severe headache appears and the lymph nodes in the neck, groin and armpits become enlarged. The patient feels completely overwhelmed, constant drowsiness and apathy.
Often, after infection in the initial stages, the patient may experience diarrhea. It may also be detected. The frequent and unexplained occurrence of such symptoms should be a reason to conduct an HIV test in a specialized center.
The first signs of AIDS in men and women
After the stage of primary manifestations of HIV, which can last about three weeks, the patient often experiences a prolonged low-grade fever. Some infected people may remain unaware of the disease for many years. Then they develop immunodeficiency, which leads to a long course of any disease.
The first signs of AIDS are the same for both men and women. Only the symptoms of diseases of the reproductive system may be different. The first sign of its onset may be long-term non-healing cuts and wounds. In such patients, even a slight scratch can bleed and fester for a long time.
- pulmonary – the patient develops Pneumocystis pneumonia, which is characterized by a long and severe course;
- intestinal - first the patient develops diarrhea, signs of dehydration, rapid and significant weight loss;
- with damage to the skin, mucous membranes and tissues of the body - the patient develops ulcers and erosions on the mucous membranes or skin, which progress, become infected and grow into muscle tissue;
- with damage to the nervous system - the patient’s memory deteriorates, constant apathy appears, brain atrophy and epileptic seizures develop, the condition can be complicated by malignant brain tumors or encephalitis.
AIDS lasts about six months or two years and ends in death (few patients live for three years).
Rapid detection of AIDS is complicated by the fact that the first signs of HIV infection are nonspecific and can be attributed to many other ailments. Frequent and unfounded appearance of temperature and enlarged lymph nodes should necessarily alert the patient and his doctor. In such cases, the only correct solution may be to conduct an HIV test in a specialized center. The need for timely diagnosis of this deadly disease is beyond doubt, since earlier initiation of antiviral therapy can delay the transition of HIV to AIDS, and therefore prolong the life of an infected person.
HIV infection (infection caused by the human immunodeficiency virus) is a global health problem, the consequences of which kill about a million people every year. For example, in 2014, 1.2 million people died from HIV-related causes. The number of people infected with HIV is in the tens of millions. In Russia, as of the end of January 2016, the number of HIV-infected people reached 1 million people.
We recommend reading:AIDS virus
At its core, HIV infection is a slowly progressive viral disease that affects the immune system, the extreme stage of development of which is AIDS (acquired immunodeficiency syndrome). Patients do not die from HIV infection itself, but the suppression of immunity that occurs under the influence of the virus leads to the fact that a person becomes unprotected against cancer and severe infectious diseases that are not dangerous for people with normal immunity.
In this regard, it is extremely important to detect HIV infection in a timely manner and begin treatment, which allows the infected person to live quite actively and productively for decades.
HIV infection is caused by a special retrovirus, the human immunodeficiency virus (HIV). which opened in 1983. It is quite unstable to physical and chemical factors when compared, for example, with hepatitis viruses. Both salivary enzymes and gastric juice are harmful to HIV. Outside the body, it quickly dies - as soon as the blood, sperm and other fluids of the human body dry out. Temperatures above 56 degrees kill this virus instantly. All these factors influence the characteristics of HIV transmission.

HIV is especially prone to attack immune system cells that have specific CD4 receptors on their surface. These cells include T-helper lymphocytes, monocytes, macrophages, dendritic and other cells. The mechanisms by which HIV affects the immune system are quite complex, but the final result is a significant decrease in the number of CD4+ lymphocytes and suppression of the immune system. 
Some people are not naturally susceptible to HIV. Their immune cells contain not normal, but partially altered proteins (CCR5) on the membrane, which is why the interaction of cells with the virus simply cannot occur. In addition, among people infected with HIV, about 1-5% are non-progressors. Their HIV infection does not progress, lymphocytes do not die, and AIDS does not develop. This phenomenon serves as an example of asymptomatic carriage, which occurs in other infectious diseases.
How does HIV infection occur?
HIV, in a concentration sufficient to infect another person, is found only in certain environments of the body: blood, pre-ejaculate, semen, vaginal secretions, milk, lymph. When these media come into contact with damaged skin and mucous membranes, or when they penetrate directly into the bloodstream of a healthy person, infection occurs. Saliva, tears and other body fluids do not pose a risk of transmitting infection, provided they do not contain blood.
Intact skin is a reliable barrier to HIV, but mucous membranes are more susceptible because they contain dendritic cells. They have CD4 receptors on their surface and can act as a carrier of a dangerous infection into the lymphatic system. Moreover, even minimal damage to the mucous membrane, which is not always noticeable to the naked eye, is already a high risk of infection. Therefore, with genital infections that provoke the development of inflammatory processes, erosions, ulcers on the genital mucosa, the penetration of HIV into the internal environment of the body is greatly simplified.

Based on all this, it can be argued that HIV infection is most likely possible in the following cases:
- When using contaminated needles. This route of transmission is especially relevant for injection drug users.
- When transfusing insufficiently tested donor blood or its components.
- During unprotected sexual intercourse (if we evaluate the level of danger, then anal sex comes first, then vaginal and oral sex). The risk of infection is always higher with the receiving partner and in the presence of concomitant sexually transmitted infections.
- During pregnancy and childbirth from a sick mother to a child.
- When breastfeeding (in newborns there are no enzymes in the saliva and gastric juice that kill HIV).
It is also worth noting that HIV is not transmitted through:
- shared dishes, bedding, etc.;
- insect bites;
- shaking hands (if there are no open wounds on the hands);
- embrace;
- air;
- food;
- water (for example, in a swimming pool);
- kissing (again, provided that both partners do not have any injuries on the lips or in the oral cavity).

At-risk groups
Some people are at particularly high risk of contracting HIV and should be tested regularly for the infection. These risk groups include:
- Injecting drug addicts and their sexual partners.
- People who practice unprotected sex (in both homosexual and heterosexual couples) and frequently change partners.
- Medical workers who, due to their professional activities, may have direct contact with the blood or mucous membranes of an infected person.
- Persons who have had blood or its components transfused.
- Children born to HIV-infected mothers.
Clinical picture

HIV infection has the following stages of development:
- Incubation period, which lasts from several days to 2-3 weeks.
- Acute phase. It usually lasts 10-14 days and most often occurs in the form of “flu-like” or “mononucleosis-like” syndromes. Patients are concerned about low-grade fever, enlarged and painful lymph nodes, pain in joints and muscles, rash on the body, ulcers on the oral mucosa, sore throat, general weakness. Nausea and diarrhea may also occur. The development of all these symptoms is associated with very active reproduction of virions in lymphoid tissue, high viral load (concentration of viruses in the blood) and a sharp drop in the number of CD4+ lymphocytes. During the acute phase, the patient is considered to be the most contagious. It is also worth noting that this phase may be asymptomatic.
- Latent period. At this stage of the disease, almost all the symptoms described above disappear, and the patient’s immune system “comes to its senses” - the number of lymphocytes increases, and for some time the body maintains them at a level that provides adequate immune protection. This period lasts 5-10 years, if the patient receives antiretroviral treatment - for decades. The only sign that in the latent period may indicate that something pathological is happening in the body is an enlargement of the lymph nodes.
- PreAIDS. This stage begins when the level of CD4+ lymphocytes drops critically and approaches 200 cells in 1 μl of blood. As a result of such suppression of the immune system (its cellular component), the patient develops: recurrent herpes and candidiasis of the oral cavity, genitals, herpes zoster, hairy leukoplakia of the tongue (whitish protruding folds and plaques on the lateral surfaces of the tongue). In general, any infectious disease (for example, tuberculosis, salmonellosis, pneumonia) is more severe than in the general population. In addition, this stage of HIV infection is characterized by a progressive decrease in the patient’s weight.
- AIDS. This is already the terminal stage of the disease, which without treatment ends in the death of a person within 1-3 years. The cause of such disastrous consequences of HIV infection are opportunistic infections (those that do not develop in people with normal immunity), severe non-communicable diseases and cancer.
The following factors can accelerate the progression of HIV infection:
- Elderly age.
- The presence of other viral diseases (for example, hepatitis).
- Poor nutrition.
- Unsatisfactory living conditions.
- Stress.
- Bad habits.
- Genetic features.
Signs of HIV infection
Assessing existing symptoms of a disease and making diagnoses is the prerogative of doctors, but every sane person should know Signs that may indicate HIV infection:
- Unreasonable prolonged increase in body temperature.
- Enlarged lymph nodes.
- Sudden unjustified weight loss.
- Prolonged diarrhea of unknown etiology.
- Tendency to chronicity and constant recurrence of bacterial and viral infectious diseases.
- The occurrence of ailments caused by opportunistic bacteria, fungi, protozoa (this indicates an immunodeficiency state).
Who needs HIV testing:

Why you need to know your HIV status:
- In case of a positive result, treatment can be started in a timely manner and the development of AIDS can be prevented.
- To prevent infection of other people if HIV infection is confirmed.
HIV testing is carried out free of charge, voluntarily (with the exception of certain categories of citizens, which in the Russian Federation include the following) and, if desired, anonymously. However, it is worth noting that the anonymous result has no legal force. For example, it cannot be attached to a pregnant woman’s exchange card or provided to migration service agencies.
You can get tested for HIV in specialized AIDS prevention and control centers, as well as in city clinics.
There are two types of HIV tests:
- Indirect, allowing to detect antibodies to the virus in the blood using ELISA (screening tests and confirmatory tests).
- Direct – detection of the virus itself, its antigens and RNA (viral load).
 HIV screening tests are quick, accessible and fairly informative tests that are used for mass screening of people. If the screening test is positive, it is repeated to rule out error. A repeated positive result requires confirmation by a more accurate, but also expensive analysis - immunoblotting.
HIV screening tests are quick, accessible and fairly informative tests that are used for mass screening of people. If the screening test is positive, it is repeated to rule out error. A repeated positive result requires confirmation by a more accurate, but also expensive analysis - immunoblotting.
In addition, with HIV infection there is such a thing as a “window” period - this is the time during which, after infection, antibodies to HIV are not detected in the patient’s blood. The duration of this period largely depends on the immune status of the person, that is, an exact figure cannot be given. However, it is believed that modern ELISA test systems can “detect” antibodies within 3-5 weeks after infection in most people. But still, in order not to make a mistake, it is advisable after the first negative examination to undergo 2 more with an interval of 3 months. In rare cases, if a person has problems with the immune system, the “window” period can last up to a year.
As for direct tests for detecting HIV, the most often used in practice is the detection of viral RNA by the polymerase chain reaction (PCR) method. This test can show that a person is infected with HIV even when they are in their window period. But a doctor cannot make a diagnosis of HIV infection based only on this result without confirmation by other tests, except in cases in which the assessment of the patient’s immune response may be incorrect. For example, in children born to HIV-positive mothers. Maternal antibodies are transferred to newborns, which will be detected in the child up to 18 months. In addition, a PCR test (determining viral load) is used during patient treatment to determine the effectiveness of the therapy received.
Treatment
We recommend reading:
There are no medications that can completely remove HIV from the human body, so this disease is considered incurable. However, highly active antiretroviral therapy (HAART) can significantly slow the progression of the infection. In addition, against the background of antiretroviral therapy, the patient becomes less infectious (this is one of the aspects of preventing HIV infection).

HAART requires the patient to take three or four antiviral drugs (acting at different stages of the virus) for life. It is very important that the patient observes the dosage and regularity of taking medications. Failure to comply with recommendations leads to the virus developing resistance to drugs, and it is necessary to switch to other, often more expensive, treatment regimens.
Drugs used in the treatment of HIV infection include the following:
- Nucleoside reverse transcriptase inhibitors (Zidovudine, Lamivudine, Tenofovir, Abacovir, etc.).
- Non-nucleoside reverse transcriptase inhibitors (Nevirapine, Etravirine, Efavirenz, etc.).
- Protease inhibitors (Amprenavir, Atazanavir, Nelfinavir, Ritonavir, etc.).
- Integrase inhibitors (Dolutegravir, Raltegravir).
- Receptor inhibitors (Maraviroc).
- Fusion inhibitors (Enfuvirtide).
It is worth noting that HAART is not prescribed to everyone infected with HIV. Patients are selected according to three main criteria: the presence of symptoms of immunodeficiency, the concentration of CD4+ lymphocytes and viral load. But in September 2015, WHO issued new recommendations that all people with HIV, as well as those at high risk of infection, should be treated with antiretroviral drugs (this preventive treatment is called pre-exposure prophylaxis). These measures, according to WHO estimates, should save tens of millions of lives and tens of millions more people from contracting a dangerous disease in the near future. WHO recommendations can be read.
Forecast
We recommend reading:Without treatment, HIV infection ends in the death of the patient on average after 9-11 years. If HAART is carried out and the patient follows all the doctor’s recommendations regarding lifestyle, bad habits, nutrition, as well as regular monitoring of health, most people with HIV can live to old age.
Prevention of HIV/AIDS
- Using condoms.
- Regular HIV testing of representatives of risk groups.
- Medical circumcision of the foreskin in men.
- Antiretroviral therapy for preventive purposes. This includes pre-exposure prophylaxis for HIV-negative partners of people with HIV and post-exposure prophylaxis after possible exposure.
- Harm reduction for injection drug users (programs to replace used syringes, opioid substitution therapy, HIV testing, etc. should be conducted).
- Eliminating mother-to-child transmission of the virus. To achieve this, all women with HIV and their newborns must be provided with antiretroviral therapy. In such situations, breastfeeding is also not recommended.

In addition, preventive measures include mandatory testing of donor blood, compliance with the appropriate regime in medical institutions, and educational work among the population.
If we talk about preventing HIV infection for a particular person, then the following rules of life should be for him: rejection of casual sex, protected sex and a negative attitude towards drugs.
The human immunodeficiency virus belongs to the group of retroviruses and provokes the development of HIV infection. This disease can occur in several stages, each of which differs in clinical picture and intensity of manifestations.
Stages of HIV
Stages of development of HIV infection:
- incubation period;
- primary manifestations are acute infection, asymptomatic and generalized lymphadenopathy;
- secondary manifestations - persistent damage to internal organs, damage to the skin and mucous membranes, generalized diseases;
- terminal stage.
According to statistics, HIV infection is most often diagnosed at the stage of secondary manifestations and this is due to the fact that the symptoms of HIV become pronounced and begin to bother the patient during this period of the disease.
At the first stage of development of HIV infection, certain symptoms may also be present, but they, as a rule, are mild, the clinical picture is blurred, and the patients themselves do not turn to doctors for such “little things.” But there is one more nuance - even if a patient seeks qualified medical help at the first stage of HIV infection, specialists may not diagnose the pathology. Moreover, at this stage of development of the disease in question, the symptoms will be the same in men and women - this often confuses doctors. And only at the secondary stage is it quite possible to hear the diagnosis of HIV infection, and the symptoms will be individual for males and females.
How long does it take for HIV to appear?
We recommend reading: The first signs of HIV infection go unnoticed, but they are there. And they appear on average from 3 weeks to 3 months after infection. A longer period is also possible.
The first signs of HIV infection go unnoticed, but they are there. And they appear on average from 3 weeks to 3 months after infection. A longer period is also possible.
Signs of secondary manifestations of the disease in question may also appear only many years after contracting HIV infection, but manifestations may also occur as early as 4-6 months from the moment of infection.
We recommend reading: After a person becomes infected with HIV, no symptoms or even small hints of the development of any pathology are observed for a long time. It is precisely this period that is called incubation; it can last, in accordance with the classification of V.I. Pokrovsky, from 3 weeks to 3 months.
After a person becomes infected with HIV, no symptoms or even small hints of the development of any pathology are observed for a long time. It is precisely this period that is called incubation; it can last, in accordance with the classification of V.I. Pokrovsky, from 3 weeks to 3 months.
No examinations or laboratory tests of biomaterials (serological, immunological, hematological tests) will help identify HIV infection, and the infected person himself does not look sick at all. But it is the incubation period, without any manifestations, that poses a particular danger - a person serves as a source of infection.
Some time after infection, the patient enters an acute phase of the disease - the clinical picture during this period may become a reason for diagnosing HIV infection as “questionable”.
The first manifestations of HIV infection in the acute phase of its course strongly resemble the symptoms of mononucleosis. They appear on average from 3 weeks to 3 months from the moment of infection. These include:

When examining a patient, a doctor can determine a slight increase in the size of the spleen and liver - the patient, by the way, may also complain of periodic pain in the right hypochondrium. The patient's skin may be covered with a small rash - pale pink spots that do not have clear boundaries. There are often complaints from infected people about long-term bowel dysfunction - they are tormented by diarrhea, which is not relieved even with specific medications and changes in diet.
Please note: during this course of the acute phase of HIV infection, increased numbers of lymphocytes/leukocytes and atypical mononuclear cells will be detected in the blood.
The above-described signs of the acute phase of the disease in question can be observed in 30% of patients. Another 30-40% of patients experience an acute phase in the development of serous meningitis or encephalitis - the symptoms will be radically different from those already described: nausea, vomiting, increased body temperature to critical levels, severe headache.
Often the first symptom of HIV infection is esophagitis - an inflammatory process in the esophagus, which is characterized by difficulty swallowing and pain in the chest area.
Whatever the form of the acute phase of HIV infection, after 30-60 days all symptoms disappear - often the patient thinks that he has been completely cured, especially if this period of pathology was practically asymptomatic or their intensity was low (and this can also be ).
 During this stage of the disease in question, there are no symptoms - the patient feels great and does not consider it necessary to appear at a medical facility for a preventive examination. But it is at the asymptomatic stage that antibodies to HIV can be detected in the blood! This makes it possible to diagnose pathology at one of the early stages of development and begin adequate, effective treatment.
During this stage of the disease in question, there are no symptoms - the patient feels great and does not consider it necessary to appear at a medical facility for a preventive examination. But it is at the asymptomatic stage that antibodies to HIV can be detected in the blood! This makes it possible to diagnose pathology at one of the early stages of development and begin adequate, effective treatment.
The asymptomatic stage of HIV infection can last several years, but only if the patient’s immune system has not been significantly damaged. The statistics are quite contradictory - only 30% of patients within 5 years after the asymptomatic course of HIV infection begin to experience symptoms of the following stages, but in some infected people the asymptomatic stage progresses rapidly, lasting no more than 30 days.
 This stage is characterized by an increase in almost all groups of lymph nodes; this process does not affect only the inguinal lymph nodes. It is noteworthy that it is generalized lymphadenopathy that can become the main symptom of HIV infection if all previous stages of development of the disease in question occurred without any manifestations.
This stage is characterized by an increase in almost all groups of lymph nodes; this process does not affect only the inguinal lymph nodes. It is noteworthy that it is generalized lymphadenopathy that can become the main symptom of HIV infection if all previous stages of development of the disease in question occurred without any manifestations.
Lymphozules increase by 1-5 cm, remain mobile and painless, and the surface of the skin above them has absolutely no signs of a pathological process. But with such a pronounced symptom as enlarged groups of lymph nodes, the standard causes of this phenomenon are excluded. And here, too, lies the danger - some doctors classify lymphadenopathy as difficult to explain.
The stage of generalized lymphadenopathy lasts 3 months, about 2 months after the start of the stage the patient begins to lose weight.
Secondary manifestations
It often happens that it is the secondary manifestations of HIV infection that serve as the basis for high-quality diagnosis. Secondary manifestations include:
 The patient notices a sudden increase in body temperature, he develops a dry, obsessive cough, which eventually turns into a wet one. The patient develops intense shortness of breath with minimal physical activity, and the patient's general condition rapidly deteriorates. Therapy carried out using antibacterial drugs (antibiotics) does not produce a positive effect.
The patient notices a sudden increase in body temperature, he develops a dry, obsessive cough, which eventually turns into a wet one. The patient develops intense shortness of breath with minimal physical activity, and the patient's general condition rapidly deteriorates. Therapy carried out using antibacterial drugs (antibiotics) does not produce a positive effect.
Generalized infection
These include herpes, tuberculosis, cytomegalovirus infection, and candidiasis. Most often, these infections affect women and, against the background of the human immunodeficiency virus, they are extremely severe.
Kaposi's sarcoma
This is a neoplasm/tumor that develops from lymphatic vessels. More often diagnosed in men, it has the appearance of multiple tumors of a characteristic cherry color located on the head, torso and in the oral cavity.
Damage to the central nervous system
At first, this manifests itself only as minor problems with memory and decreased concentration. But as the pathology progresses, the patient develops dementia.
Features of the first signs of HIV infection in women
 If a woman is infected with the human immunodeficiency virus, then secondary symptoms will most likely manifest themselves in the form of development and progression of generalized infections - herpes, candidiasis, cytomegalovirus infection, tuberculosis.
If a woman is infected with the human immunodeficiency virus, then secondary symptoms will most likely manifest themselves in the form of development and progression of generalized infections - herpes, candidiasis, cytomegalovirus infection, tuberculosis.
Often, secondary manifestations of HIV infection begin with a banal menstrual cycle disorder; inflammatory processes in the pelvic organs, for example, salpingitis, can develop. Oncological diseases of the cervix - carcinoma or dysplasia - are also often diagnosed.
Features of HIV infection in children
 Children who were infected with the human immunodeficiency virus during pregnancy (in utero from the mother) have some features in the course of the disease. Firstly, the disease begins its development at 4-6 months of life. Secondly, the earliest and main symptom of HIV infection during intrauterine infection is considered to be a disorder of the central nervous system - the baby lags behind his peers in physical and mental development. Thirdly, children with the human immunodeficiency virus are susceptible to the progression of digestive system disorders and the appearance of purulent diseases.
Children who were infected with the human immunodeficiency virus during pregnancy (in utero from the mother) have some features in the course of the disease. Firstly, the disease begins its development at 4-6 months of life. Secondly, the earliest and main symptom of HIV infection during intrauterine infection is considered to be a disorder of the central nervous system - the baby lags behind his peers in physical and mental development. Thirdly, children with the human immunodeficiency virus are susceptible to the progression of digestive system disorders and the appearance of purulent diseases.
The human immunodeficiency virus is still an unexplored disease - too many questions arise both during diagnosis and treatment. But doctors say that only patients themselves can detect HIV infection at an early stage - they are the ones who must closely monitor their health and periodically undergo preventive examinations. Even if the symptoms of HIV infection are hidden, the disease develops - only a timely test analysis will help save the patient’s life for several years.
Answers to popular questions about HIV
Due to the large number of requests from our readers, we decided to group the most common questions and answers to them in one section.
Signs of HIV infection appear approximately 3 weeks to 3 months after dangerous contact. An increase in temperature, sore throat and enlarged lymph nodes in the first days after infection may indicate any pathology other than the human immunodeficiency virus. During this period (doctors call it incubation), not only are there no symptoms of HIV, but in-depth laboratory blood tests will not give a positive result.
Yes, unfortunately, this is rare, but it does happen (in about 30% of cases): a person does not notice any characteristic symptoms during the acute phase, and then the disease goes into the latent phase (this is, in fact, an asymptomatic course for about 8 - 10 years ).
Most modern screening tests are based on enzyme-linked immunosorbent assay (ELISA) - this is the “gold standard” for diagnosis, and an accurate result can be counted on no earlier than 3 to 6 months after infection. Therefore, the test must be taken twice: 3 months after possible infection and then another 3 months later.
Firstly, you need to take into account the period that has passed since the potentially dangerous contact - if less than 3 weeks have passed, then these symptoms may indicate a common cold.
Secondly, if more than 3 weeks have already passed since the possible infection, then you should not stress yourself out - just wait and 3 months after the dangerous contact undergo a specific examination.
Thirdly, increased body temperature and enlarged lymph nodes are not “classic” signs of HIV infection! Often the first manifestations of the disease are expressed by pain in the chest and a burning sensation in the esophagus, stool disturbances (the person is bothered by frequent diarrhea), and a pale pink rash on the skin.
The risk of contracting HIV infection through oral sex is minimized. The fact is that the virus does not survive in the environment, so in order to be infected orally, two conditions must come together: there are wounds/abrasions on the partner’s penis and wounds/abrasions in the partner’s mouth. But even these circumstances do not in every case lead to HIV infection. For your own peace of mind, you need to take a specific HIV test 3 months after dangerous contact and undergo a “control” examination after another 3 months.
There are a number of medications that are used for post-exposure prophylaxis for HIV. Unfortunately, they are not available for sale, so you will have to go to an appointment with a therapist and explain the situation. There is no guarantee that such measures will 100% prevent the development of HIV infection, but experts say that taking such medications is quite advisable - the risk of developing the human immunodeficiency virus is reduced by 70-75%.
If there is no opportunity (or courage) to consult a doctor with a similar problem, then there is only one thing left to do - wait. You will need to wait 3 months, then undergo an HIV test, and even if the result is negative, you should take a control test after another 3 months.
No you can not! The human immunodeficiency virus does not survive in the environment, therefore, with people who are classified as HIV-positive, you can without hesitation share dishes, bed linen, and visit the pool and sauna.
There are risks of infection, but they are quite small. So, with a single vaginal sexual intercourse without a condom, the risk is 0.01 - 0.15%. With oral sex, the risks range from 0.005 to 0.01%, with anal sex - from 0.065 to 0.5%. These statistics are provided in the clinical protocols for the WHO European Region for HIV/AIDS treatment and care (page 523).
Cases have been described in medicine where married couples, where one of the spouses was HIV-infected, lived sexually without using condoms for several years, and the second spouse remained healthy.
If a condom was used during sexual intercourse, it was used according to instructions and remained intact, then the risk of becoming infected with HIV is minimized. If, 3 or more months after the questionable contact, symptoms reminiscent of HIV infection appear, then you just need to consult a therapist. An increase in temperature and enlarged lymph nodes may indicate the development of ARVI and other diseases. For your own peace of mind, you should get tested for HIV.
To answer this question, you need to know at what time and how many times such an analysis was taken:
- a negative result in the first 3 months after dangerous contact cannot be accurate; doctors talk about a false negative result;
- a negative HIV test response after 3 months from the moment of dangerous contact - most likely the person being examined is not infected, but another test must be done 3 months after the first for control;
- negative HIV test response 6 months or more after dangerous contact - the subject is not infected.
The risks in this case are extremely small - the virus quickly dies in the environment, therefore, even if the blood of an infected person remains on the needle, it is almost impossible to become infected with HIV by being injured by such a needle. There cannot be a virus in dried biological fluid (blood). However, after 3 months, and then again - after another 3 months - it is still worth taking an HIV test.
Tsygankova Yana Aleksandrovna, medical observer, therapist of the highest qualification category.
 Now in the world, perhaps, there is no adult who does not know what HIV infection is. The “plague of the 20th century” has confidently stepped into the 21st century and continues to progress. The prevalence of HIV is now in the nature of a real pandemic. HIV infection has spread to almost all countries. In 2004, there were about 40 million people living with HIV in the world – approximately 38 million adults and 2 million children. In the Russian Federation, the prevalence of HIV-infected people in 2003 was 187 people per 100 thousand population.
Now in the world, perhaps, there is no adult who does not know what HIV infection is. The “plague of the 20th century” has confidently stepped into the 21st century and continues to progress. The prevalence of HIV is now in the nature of a real pandemic. HIV infection has spread to almost all countries. In 2004, there were about 40 million people living with HIV in the world – approximately 38 million adults and 2 million children. In the Russian Federation, the prevalence of HIV-infected people in 2003 was 187 people per 100 thousand population.
According to statistics, about 8,500 people are infected every day in the world, with at least 100 in Russia.
Basic concepts:
HIV– human immunodeficiency virus – the causative agent of HIV infection.
– an infectious disease whose cause is HIV and the outcome is AIDS.
AIDS– acquired immunodeficiency syndrome is the final stage of HIV infection, when a person’s immune system is so damaged that it becomes unable to resist any type of infection. Any infection, even the most harmless one, can lead to severe illness and death.

History of HIV infection
In the summer of 1981, the US Centers for Disease Control published a report describing 5 cases of Pneumocystis pneumonia and 26 cases of Kaposi's sarcoma in previously healthy homosexual men from Los Angeles and New York.
Over the next few months, cases were reported among injecting drug users and, shortly thereafter, among blood transfusion recipients.
In 1982, the diagnosis of AIDS was formulated, but the causes of its occurrence were not established.
In 1983, it was first allocated HIV from a cell culture of a sick person.
In 1984 it was found that HIV is the reason AIDS.
In 1985, a diagnostic method was developed HIV infection using an enzyme-linked immunosorbent assay (ELISA) that detects antibodies to HIV in blood.
In 1987, the first case HIV infection registered in Russia - he was a homosexual man who worked as a translator in African countries.
Where did HIV come from?
In search of an answer to this question, many different theories have been proposed. No one can answer this for sure.
However, it is known that the first study of the epidemiology of HIV infection found that the maximum prevalence of HIV was in the Central African region. In addition, a virus capable of causing AIDS in humans has been isolated from the blood of the great apes (chimpanzees) living in this area, which may indicate the possibility of infection from these apes, perhaps through a bite or butchering of carcasses.
There is an assumption that HIV existed for a long time among the tribal settlements of Central Africa, and only in the twentieth century, as a result of increased population migration, it spread throughout the world.
AIDS virus
HIV (human immunodeficiency virus) belongs to a subfamily of retroviruses called lentiviruses (or “slow” viruses). This means that from the moment of infection to the appearance of the first signs of the disease, and especially to the development of AIDS, a long period of time passes, sometimes several years. Half of HIV-infected people have an asymptomatic period of about 10 years.
There are 2 types of HIV - HIV-1 and HIV-2. The most common virus in the world is HIV-1; HIV-2 is closer in morphology to the simian immunodeficiency virus - the same one that was found in the blood of chimpanzees.
* - In 2019, a group of scientists in the United States discovered a new strain of HIV for the first time in almost 20 years. This strain is part of the group M species of HIV-1. There are many different subtypes or strains of HIV. Like other viruses, it can change and mutate over time. This is the first new group M strain discovered since subtype classification principles were established in 2000.
When HIV enters the blood, it selectively attaches to blood cells responsible for immunity, which is due to the presence on the surface of these cells of specific CD 4 molecules that HIV recognizes. Inside these cells, HIV actively multiplies and, even before the formation of any immune response, quickly spreads throughout the body. It primarily affects the lymph nodes, since they contain a large number of immune cells.
Throughout the course of the disease, an effective immune response to HIV is never formed. This is primarily due to damage to immune cells and insufficiency of their function. In addition, HIV has pronounced variability, which leads to the fact that immune cells simply cannot “recognize” the virus.
As the disease progresses, HIV leads to damage to an increasing number of immune cells - CD 4 lymphocytes, the number of which gradually decreases, eventually reaching a critical number, which can be considered the beginning AIDS.
How can you become infected with HIV?
- During sexual intercourse.
Sexual transmission is the most common route of HIV transmission worldwide. Semen contains large amounts of virus; Apparently, HIV tends to accumulate in semen, especially in inflammatory diseases - urethritis, epididymitis, when semen contains a large number of inflammatory cells containing HIV. Therefore, the risk of HIV transmission increases with concomitant sexually transmitted infections. In addition, concomitant genital infections are often accompanied by the appearance of various formations that violate the integrity of the mucous membrane of the genital organs - ulcers, cracks, blisters, etc.
HIV is also found in vaginal and cervical discharge.
You should also remember about the criminal liability (Article 122 of the Criminal Code of the Russian Federation), which is borne by an HIV-positive partner, putting the other in a situation dangerous from the point of view of contracting HIV infection. In the same article. 122 a note has been added on the basis of which a person is exempt from criminal liability if the partner was promptly warned about the presence of HIV infection and voluntarily agreed to commit actions that created a risk of infection.
During anal intercourse, the risk of transmitting the virus from semen through the thin mucous membrane of the rectum is extremely high. In addition, during anal sex, the risk of injury to the rectal mucosa increases, which means direct contact with blood.
In heterosexual contacts, the risk of infection from a man to a woman is approximately 20 times higher than from a woman to a man. This is due to the fact that the duration of contact of the vaginal mucosa with infected sperm is much longer than the duration of contact of the penis with the vaginal mucosa.
With oral sex, the risk of infection is much lower than with anal sex. However, it has been reliably proven that this risk does occur! Using condoms reduces, but does NOT eliminate, HIV infection.
- When using the same syringes or needles among injection drug users.
- During transfusion of blood and its components.
You cannot become infected by administering normal immunoglobulin and specific immunoglobulins, since these drugs undergo special treatment to completely inactivate the virus. After the introduction of mandatory testing of donors for HIV , the risk of infection has decreased significantly; however, the presence of a “blind period”, when the donor is already infected, but antibodies have not yet formed, does not completely protect recipients from infection.
- From mother to child.
Infection of the fetus can occur during pregnancy - the virus is able to penetrate the placenta; and also during childbirth. The risk of infection of a child from an HIV-infected mother is 12.9% in European countries and reaches 45-48% in African countries. The risk depends on the quality of the mother's medical care and treatment during pregnancy, the mother's health status, and the stage of HIV infection.
In addition, there is a clear risk of infection during breastfeeding. The virus has been found in the colostrum and breast milk of HIV-infected women. That's why is a contraindication for breastfeeding.
- From patients to medical staff and vice versa.
The risk of infection when injured by sharp objects contaminated with the blood of HIV-infected people is about 0.3%. The risk of contact of infected blood with mucous membranes and damaged skin is even lower.
The risk of HIV transmission from an infected healthcare worker to a patient is theoretically difficult to imagine. However, in 1990, a report was published in the United States about the infection of 5 patients from an HIV-infected dentist, but the mechanism of infection remained a mystery. Subsequent observations of patients who were treated by HIV-infected surgeons, gynecologists, obstetricians, and dentists did not reveal a single fact of infection.
How not to become infected with HIV
If there is an HIV-infected person in your environment, you must remember that you cannot become infected HIV at:
- Coughing and sneezing.
- Handshake.
- Hugs and kisses.
- Consumption of shared food or drinks.
- In swimming pools, baths, saunas.
- Through “injections” in transport and the metro. Information about possible infection through infected needles that HIV-infected people place on seats, or try to inject people in a crowd with them, is nothing more than myths. The virus does not persist in the environment for very long; in addition, the virus content at the tip of the needle is too small.
Saliva and other biological fluids contain too little virus to cause infection. The risk of infection occurs if body fluids (saliva, sweat, tears, urine, feces) contain blood.
Symptoms of HIV
Acute febrile phase
The acute febrile phase appears approximately 3-6 weeks after infection. It does not occur in all patients - approximately 50-70%. The rest immediately enter an asymptomatic phase after the incubation period.
Manifestations of the acute febrile phase are nonspecific:
- Fever: increased temperature, often low-grade fever, i.e. not higher than 37.5ºС.
- Sore throat.
- Enlarged lymph nodes: the appearance of painful swellings in the neck, armpits, and groin.
- Headache, eye pain.
- Pain in muscles and joints.
- Drowsiness, malaise, loss of appetite, weight loss.
- Nausea, vomiting, diarrhea.
- Skin changes: skin rash, ulcers on the skin and mucous membranes.
- Serous meningitis can also develop - damage to the membranes of the brain, which is manifested by headache and photophobia.
The acute phase lasts from one to several weeks. In most patients it is followed by an asymptomatic phase. However, approximately 10% of patients experience a fulminant course of HIV infection with a sharp deterioration in their condition.
Asymptomatic phase of HIV infection
The duration of the asymptomatic phase varies widely - in half of HIV-infected people it is 10 years. The duration depends on the rate of virus reproduction.
During the asymptomatic phase, the number of CD 4 lymphocytes progressively decreases; a drop in their level below 200/μl indicates the presence of AIDS.
The asymptomatic phase may not have any clinical manifestations.
Some patients have lymphadenopathy – i.e. enlargement of all groups of lymph nodes.
Advanced stage of HIV - AIDS
At this stage, the so-called opportunistic infections– these are infections caused by opportunistic microorganisms that are normal inhabitants of our body and under normal conditions are not capable of causing disease.
There are 2 stages of AIDS:
A. Decrease in body weight by 10% compared to the original.
Fungal, viral, bacterial infections of the skin and mucous membranes:
- Candidal stomatitis: thrush is a white cheesy coating on the oral mucosa.
- Hairy leukoplakia of the mouth is white plaques covered with grooves on the lateral surfaces of the tongue.
- Shingles is a manifestation of the reactivation of the varicella zoster virus, the causative agent of chickenpox. It manifests itself as severe pain and rashes in the form of blisters on large areas of the skin, mainly the torso.
- Repeated frequent occurrences of herpetic infection.
In addition, patients constantly suffer from pharyngitis (sore throat), sinusitis (sinusitis, phronitis), and otitis (inflammation of the middle ear).
Bleeding gums, hemorrhagic rash (bleeding) on the skin of the hands and feet. This is associated with developing thrombocytopenia, i.e. a decrease in the number of platelets - blood cells involved in clotting.
B. Decrease in body weight by more than 10% from the original.
At the same time, others are added to the infections described above:
- Unexplained diarrhea and/or fever for more than 1 month.
- Tuberculosis of the lungs and other organs.
- Toxoplasmosis.
- Helminthiasis of the intestines.
- Pneumocystis pneumonia.
- Kaposi's sarcoma.
- Lymphomas.
In addition, severe neurological disorders occur.
When to suspect HIV infection
- Fever of unknown origin for more than 1 week.
- Enlargement of various groups of lymph nodes: cervical, axillary, inguinal - for no apparent reason (no inflammatory diseases), especially if lymphadenopathy does not go away within several weeks.
- Diarrhea for several weeks.
- The appearance of signs of candidiasis (thrush) of the oral cavity in an adult.
- Extensive or atypical localization of herpetic eruptions.
- A sharp decrease in body weight, regardless of any reason.
Who is at higher risk of contracting HIV?
- Injection drug addicts.
- Homosexuals.
- Prostitutes.
- Persons who practice anal sex.
- People who have multiple sexual partners, especially if they do not use condoms.
- Persons suffering from other sexually transmitted diseases.
- Persons requiring transfusions of blood and its components.
- Persons requiring hemodialysis (“artificial kidney”).
- Children whose mothers are infected.
- Medical workers, especially those in contact with HIV-infected patients.
Prevention of HIV infection
Unfortunately, to date, no effective vaccine against HIV has been developed, although many countries are now conducting thorough research in this area, which has high hopes.
However, so far the prevention of HIV infection comes down to only general preventive measures:
- Safe sex and a permanent, reliable sexual partner.
Using condoms helps reduce the risk of infection, but even when used correctly, a condom is never 100% effective.
Rules for using a condom:
- The condom must be the right size.
- It is necessary to use a condom from the very beginning of sexual intercourse until completion.
- the use of condoms with nonoxynol-9 (spermicide) does not reduce the risk of infection, since it often leads to irritation of the mucous membrane, and, consequently, to microtraumas and cracks, which only contributes to infection.
- There should be no air left in the seminal receptacle - this may cause the condom to rupture.
If sexual partners want to be sure there is no risk of infection, they should both be tested for HIV.
- Quitting drug use. If it is impossible to cope with addiction, you should use only disposable needles and never share needles or syringes.
- HIV-infected mothers should avoid breastfeeding.
Drug prophylaxis has been developed for suspected HIV infection. It consists of taking antiretroviral drugs, as in the treatment of patients with HIV, only in different dosages. A course of preventive treatment will be prescribed by a doctor at the AIDS center during an in-person visit.
HIV test
Early diagnosis of HIV is extremely important for successful treatment and increasing life expectancy in such patients.
When should you get tested for HIV?
- after sexual intercourse (vaginal, anal or oral) with a new partner without a condom (or if the condom breaks). after sexual violence.
- if your sexual partner has had sex with someone else.
- if your current or past sexual partner is HIV positive.
- after using the same needles or syringes to inject drugs or other substances, or for tattoos and piercings.
- after any contact with the blood of an HIV-infected person.
- if your partner has shared needles or been exposed to any other risk of infection.
- after detection of any other sexually transmitted infection.
Most often, the diagnosis of HIV infection is carried out using methods that determine antibodies to HIV in the blood - i.e. specific proteins that are formed in the body of an infected person in response to the virus. Antibody formation occurs within 3 weeks to 6 months after infection. Therefore, an HIV test becomes possible only after this period of time; the final test is recommended to be performed 6 months after the suspected infection. Standard method for determining antibodies to HIV called enzyme immunoassay (ELISA) or ELISA. This method is very reliable, with a sensitivity of more than 99.5%. Test results may be positive, negative or inconclusive.
If the result is negative and there is no suspicion of recent (within the last 6 months) infection, the diagnosis of HIV can be considered unconfirmed. If there is a suspicion of recent infection, a repeat examination is carried out.
There is a problem with so-called false positive results, so when a positive or questionable answer is received, the result is always checked using a more specific method. This method is called immunoblotting. The result can also be positive, negative or doubtful. If a positive result is obtained, the diagnosis of HIV infection is considered confirmed. If the answer is questionable, a repeat study is required after 4-6 weeks. If the result of repeated immunoblotting remains equivocal, the diagnosis of HIV infection is unlikely. However, to completely exclude it, immunoblotting is repeated 2 more times with an interval of 3 months or other diagnostic methods are used.
In addition to serological methods (i.e., determination of antibodies), there are methods for direct detection of HIV, which can be used to determine the DNA and RNA of the virus. These methods are based on PCR (polymerase chain reaction) and are very accurate methods for diagnosing infectious diseases. PCR can be used for early diagnosis of HIV - 2-3 weeks after questionable contact. However, due to the high cost and the large number of false-positive results due to contamination of the test samples, these methods are used in cases where standard methods cannot confidently diagnose or exclude HIV.
Video about what HIV tests you need to take and why:
Drug treatment of HIV infection and AIDS
Treatment consists of prescribing antiviral – antiretroviral therapy; as well as in the treatment and prevention of opportunistic infections.
After diagnosis and registration, a series of studies are carried out to determine the stage and activity of the disease. An important indicator of the stage of the process is the level of CD 4 lymphocytes - the very cells that affect HIV, and the number of which is progressively decreasing. When the CD 4 lymphocyte count is less than 200/μl, the risk of opportunistic infection, and therefore AIDS becomes significant. In addition, to determine the progression of the disease, the concentration of viral RNA in the blood is determined. Diagnostic tests must be carried out regularly, since the course HIV infection it is difficult to predict, and early diagnosis and treatment of concomitant infections is the basis for prolonging life and improving its quality.
Antiretroviral drugs:
The prescription of antiretroviral drugs and the choice of a specific drug is a decision of a medical specialist, which he makes depending on the patient’s condition.
- Zidovudine (Retrovir) is the first antiretroviral drug. Currently, zidovudine is prescribed in combination with other drugs when the CD 4 lymphocyte count is below 500/μl. Zidovudine monotherapy is prescribed only to pregnant women to reduce the risk of infection of the fetus.
Side effects: impaired hematopoietic function, headache, nausea, myopathy, liver enlargement
- Didanosine (Videx) – used in the first stage of treatment HIV and after long-term treatment with zidovudine. More often, didanosine is used in combination with other drugs.
Side effects: pancreatitis, peripheral neuritis with severe pain, nausea, diarrhea.
- Zalcitabine (Khivid) is prescribed for ineffectiveness or intolerance of zidovudine, as well as in combination with zidovudine at the initial stage of treatment.
Side effects: peripheral neuritis, stomatitis.
- Stavudin – used in adults in later stages HIV infection.
Side effects: peripheral neuritis.
- Nevirapine and delavirdine: prescribed in combination with other antiretroviral drugs in adult patients when signs of progression occur HIV infection.
Side effects: maculopapular rash, which usually goes away on its own and does not require discontinuation of the drug.
- Saquinavir is a drug belonging to the group of protease inhibitors HIV. The first drug from this group approved for use. Saquinavir is used in later stages HIV infection in combination with the above antiretroviral drugs.
Side effects: headache, nausea and diarrhea, increased liver enzymes, increased blood sugar levels.
- Ritonavir is a drug approved for use both as monotherapy and in combination with other antiretroviral drugs.
Side effects: nausea, diarrhea, abdominal pain, lip paresthesia.
- Indinavir – used to treat HIV infection in adult patients.
Side effects: urolithiasis, increased blood bilirubin.
- Nelfinavir is approved for use in both adults and children.
The main side effect is diarrhea, which occurs in 20% of patients.
Antiretroviral drugs should be provided free of charge to patients registered at the AIDS center. In addition to antiretroviral drugs, treatment HIV infection lies in the adequate selection of antimicrobial, antiviral, antifungal, and antitumor agents for the treatment of manifestations and complications AIDS.
Prevention of opportunistic infections
Prevention of opportunistic infections helps to increase the duration and improve the quality of life of patients AIDS m.
- Prevention of tuberculosis: for the timely detection of persons infected with Mycobacterium tuberculosis, all HIV-infected persons are given a Mantoux test annually. In case of a negative reaction (i.e. in the absence of an immune response to tuberculin), it is recommended to take anti-tuberculosis drugs for a year.
- Prevention of Pneumocystis pneumonia is carried out for all HIV-infected people with a decrease in CD 4 lymphocytes below 200/μl, as well as with fever of unknown origin with a temperature above 37.8ºC that persists for more than 2 weeks. Prevention is carried out with biseptol.
Opportunistic infections– these are infections caused by opportunistic microorganisms that are normal inhabitants of our body, and under normal conditions are not capable of causing disease.
- Toxoplasmosis - the causative agent is Toxoplasma gondii. The disease manifests itself as toxoplasma encephalitis, i.e. damage to the brain substance, with the development of epileptic seizures, hemiparesis (paralysis of half the body), aphasia (lack of speech). Confusion, daze, and coma may also occur.
- Intestinal helminthiasis - the causative agents are many helminths (worms). In patients AIDS can lead to severe diarrhea and dehydration.
- Tuberculosis . Mycobacterium tuberculosis is common even among healthy individuals, but they can cause disease only if the immune system is impaired. This is why most HIV-infected people are prone to developing active tuberculosis, including its severe forms. In approximately 60-80% of HIV-infected people, tuberculosis affects the lungs, and in 30-40% it affects other organs.
- Bacterial pneumonia . The most common pathogens are Staphylococcus aureus and pneumococcus. Often pneumonia is severe with the development of generalized forms of infection, i.e. entry and proliferation of bacteria in the blood - sepsis.
- Intestinal infections – salmonellosis, dysentery, typhoid fever. Even mild forms of the disease, which go away without treatment in healthy people, last a long time in HIV-infected people with numerous complications, prolonged diarrhea and generalization of the infection.
- Syphilis – In HIV-infected people, complex and rare forms of syphilis such as neurosyphilis and syphilitic nephritis (kidney damage) are more common. Complications of syphilis develop faster in AIDS patients, sometimes even with intensive treatment.
- Pneumocystis pneumonia . The causative agent of Pneumocystis pneumonia is a normal inhabitant of the lungs, but with decreased immunity it can cause severe pneumonia. The causative agent is usually classified as a fungus. Pneumocystis pneumonia develops at least once in 50% of HIV-infected people. Typical symptoms of Pneumocystis pneumonia are: fever, cough with a small amount of sputum, chest pain that gets worse with inspiration. Subsequently, shortness of breath during physical activity and weight loss may occur.
- Candidiasis is the most common fungal infection in HIV-infected people, since the causative agent, the fungus Candida albicans, is normally found in large quantities on the mucous membranes of the mouth, nose, and genitourinary tract. In one form or another, candidiasis occurs in all HIV-infected patients. Candidiasis (or thrush) manifests itself as a white, cheesy coating on the palate, tongue, cheeks, throat, and vaginal discharge. In later stages of AIDS, candidiasis of the esophagus, trachea, bronchi and lungs is possible.
- Cryptococcosis is the leading cause of meningitis (inflammation of the meninges) among HIV-infected patients. The causative agent, a yeast fungus, enters the body through the respiratory tract, but in most cases affects the brain and its membranes. Manifestations of cryptococcosis include: fever, nausea and vomiting, impaired consciousness, headache. There are also pulmonary forms of cryptococcal infection - which are accompanied by cough, shortness of breath, and hemoptysis. In more than half of patients, the fungus penetrates and multiplies in the blood.
- Herpetic infection. HIV-infected people are characterized by frequent relapses of herpes of the face, oral cavity, genitals and perianal area. As the disease progresses, the frequency and intensity of relapses increases. Herpetic lesions do not heal for a long time and lead to extremely painful and extensive damage to the skin and mucous membranes.
- Hepatitis – more than 95% of HIV-infected people are infected with the hepatitis B virus, many of them are also concomitantly infected with the hepatitis D virus. Active hepatitis B is rare in HIV-infected people, but hepatitis D in these patients is severe.
Neoplasms in HIV infection
In addition to an increased susceptibility to infections, patients AIDS the tendency to form both benign and malignant tumors increases, since tumors are also controlled by the immune system, in particular CD4 lymphocytes.
- Kaposi's sarcoma is a vascular tumor that can affect the skin, mucous membranes and internal organs. The clinical manifestations of Kaposi's sarcoma are varied. Initial manifestations appear as small red-purple nodules raised above the surface of the skin, most often occurring in exposed areas most exposed to direct sunlight. As the nodes progress, they can merge, disfiguring the skin and, if located on the legs, limiting physical activity. Of the internal organs, Kaposi's sarcoma most often affects the gastrointestinal tract and lungs, but sometimes the brain and heart.
- Lymphomas are late manifestations HIV infection. Lymphomas can affect both the lymph nodes and internal organs, including the brain and spinal cord. Clinical manifestations depend on the location of the lymphoma, but are almost always accompanied by fever, weight loss, and night sweats. Lymphomas can manifest as rapidly growing mass formations in the oral cavity, epileptic seizures, headaches, etc.
- Other malignancies occur in HIV-infected people with the same frequency as in the general population. However, in patients HIV they have a rapid course and are difficult to treat.
Neurological disorders
- AIDS dementia syndrome;
Dementia is a progressive decline in intelligence, which is manifested by impaired attention and ability to concentrate, memory deterioration, difficulty reading and solving problems.
In addition, manifestations of AIDS dementia syndrome are motor and behavioral disorders: impaired ability to maintain a certain posture, difficulty walking, tremor (twitching of various parts of the body), apathy.
In the later stages of AIDS dementia syndrome, urinary and fecal incontinence may occur, and in some cases a vegetative state develops.
Severe AIDS-dementia syndrome develops in 25% of HIV-infected people.
The cause of the syndrome has not been definitively established. It is believed to be caused by the direct effect of the virus on the brain and spinal cord.
- Epileptic seizures;
The causes of epileptic seizures can be opportunistic infections affecting the brain, neoplasms or AIDS dementia syndrome.
The most common causes are: toxoplasma encephalitis, brain lymphoma, cryptococcal meningitis and AIDS dementia syndrome.
- Neuropathy;
A common complication of HIV infection that can occur at any stage. Clinical manifestations are varied. In the early stages, it can occur in the form of progressive muscle weakness and minor sensory impairment. In the future, the manifestations may progress, including burning pain in the legs.
Living with HIV
Positive HIV test... What to do about it? How to react? How to live further?
First, try to overcome panic as quickly as possible. Yes, AIDS fatal disease, but before development AIDS you can live 10, or even 20 years. In addition, scientists all over the world are now actively searching for effective drugs; many recently developed drugs actually significantly prolong life and improve the well-being of patients AIDS. Nobody knows what science in this area will reach in 5-10 years.
WITH HIV you need to learn to live. Unfortunately, life will never be the same again. For a long time (possibly many years), no signs of illness may appear; the person feels completely healthy and full of strength. But we should not forget about infection.
First of all, you need to protect your loved ones - they must know about infection. It can be very difficult to tell your parents or loved one about HIV-positive analysis. But no matter how difficult it may be, loved ones should not be at risk, so your partner(s) (both current and former) must be informed of the test result.
Any sex, even with a condom, can be dangerous in terms of transmitting the virus, even if sometimes the risk is extremely small. Therefore, when a new partner appears, you need to give the person the opportunity to make his own choice. We must remember that not only vaginal or anal sex can be dangerous, but also oral sex.
Medical supervision:
Although there may be no signs of illness, regular monitoring of the condition is required. Typically this control is carried out in specialized AIDS-centers. Timely detection of disease progression and onset of development AIDS, and, therefore, timely treatment is the basis for successful treatment in the future and slowing down the progression of the disease. The level of CD 4 lymphocytes is usually monitored, as well as the level of viral replication. In addition, the general condition of the patient and the possible presence of opportunistic infections are assessed. Normal indicators of the state of immunity allow us to exclude the presence AIDS, which means they allow you to lead a normal life and not be afraid of any runny nose.
Pregnancy:
Most people become infected HIV In young age. Many women want to have children. They feel absolutely healthy and able to give birth and raise a child. No one can prohibit the birth of a child - this is the mother’s personal matter. However, before planning a pregnancy, you need to weigh the pros and cons. After all, HIV is most likely transmitted through the placenta, as well as during childbirth through the birth canal. Is it worth exposing a child to congenital carriage of HIV, growth under constant medical supervision, and taking toxic drugs? Even if the child does not become infected, he risks being left without parents before reaching adulthood... If the decision is nevertheless made, you need to treat pregnancy planning and pregnancy with full responsibility and, even before pregnancy, contact a doctor at the AIDS center, who will guide your actions and review treatment.
Life with AIDS:
When the CD 4 count falls below 200/μL, an opportunistic infection occurs or any other sign of a decreased immune response is diagnosed AIDS. Such people should follow a number of rules.
- Proper nutrition: You should not follow any diet, any malnutrition can be harmful. Nutrition should be high in calories and balanced.
- Give up bad habits: alcohol and smoking
- Moderate physical exercise can have a positive effect on the immune status of HIV-infected people
- You should discuss the possibility of vaccinations against certain infections with your healthcare provider. Not all vaccines can be used in people living with HIV. In particular, live vaccines should not be used. However, killed and particulate vaccines are suitable for many people with HIV, depending on their immune status.
- It is always necessary to pay attention to the quality of food and water consumed. Fruits and vegetables must be thoroughly washed with boiled water, food must be heat-treated. Untested water must be disinfected; in some countries with hot climates, even tap water can be contaminated.
- Communication with animals: it is better to exclude any contact with unfamiliar (especially homeless) animals. At the very least, you should definitely wash your hands after touching an animal, even your own. You need to look after your pet especially carefully: try to prevent it from interacting with other animals and do not allow it to touch garbage on the street. After a walk, be sure to wash it, preferably with gloves. It is also better to wear gloves when cleaning up after an animal.
- Try to limit your communication with sick or cold people. If communication is necessary, you should use a mask and wash your hands after contact with sick people.
AIDS virus(abbreviation HIV) was discovered in 1983 while researching the causes of AIDS - syndrome immunodeficiency. The first official publications about AIDS appeared back in 1981; the new disease was associated with sarcoma Kaposi and unusual pneumonia in homosexuals. The designation AIDS (AIDS) was established as a term in 1982, when similar symptoms identified in drug addicts, homosexuals and patients with hemophilia were combined into a single acquired immune deficiency syndrome.
Modern definition of HIV infection: a viral disease based on immunodeficiency, which causes the development of concomitant (opportunistic) infections and oncological processes.
AIDS is the last stage of HIV infection, congenital or acquired.
How can you become infected with HIV?
The source of infection is an HIV-infected person, at any stage of the disease and for life. Large quantities of the virus are contained in blood (including menstrual fluid) and lymph, semen, saliva, vaginal secretions, breast milk, liquor– cerebrospinal fluid, tears. Endemic(with reference to location) an HIV outbreak has been identified in West Africa; monkeys are infected with type 2 virus. No natural site of type 1 virus has been found. HIV is transmitted only from person to person.
During unprotected sexual intercourse the possibility of contracting HIV increases if there is inflammation, microtrauma of the skin or mucous membranes of the genitals, anus. At the only one Infection occurs rarely during sexual intercourse, but with each subsequent sexual intercourse the likelihood increases. During any type of intercourse receiving the sexual partner is at greater risk of acquiring HIV (from 1 to 50 per 10,000 episodes of unprotected sex) than the transmitting partner (0.5 – 6.5). Therefore, the risk group includes prostitutes with their clients and "barebackers"– gays who deliberately do not use condoms.

HIV transmission routes
A child can become infected with HIV in utero from an infected mother, if there are defects in the placenta and the virus enters the blood of the fetus. During childbirth, infection occurs through the injured birth canal, and later through breast milk. From 25 to 35% of children born to HIV-infected mothers may become carriers of the virus or develop AIDS.
For medical reasons: transfusion of whole blood and cell mass (platelets, red blood cells), fresh or frozen plasma to patients. Among medical personnel, accidental injections with a contaminated needle account for 0.3-0.5% of all cases of HIV infection, so doctors are considered a risk group.
With intravenous injections with a “public” needle or syringe, the risk of contracting HIV is more than 95%, therefore at the moment the majority of carriers of the virus and an inexhaustible source of infection are drug addicts, constituting the main risk group for HIV.
HIV CANNOT be contracted through everyday contact. as well as through water in pools and baths, insect bites, air.
Spread of HIV
Features are a variable incubation period, unequal speed of onset and severity of symptoms, which directly depend on the state of human health. People weakened(asocials, drug addicts, residents of poor countries) or with accompanying chronic or acute STDs(, etc.), get sick more often and more severely, HIV symptoms appear faster, and life expectancy is 10-11 years from the moment of infection.
In a prosperous social environment, in practically healthy people, the incubation period can last 10-20 years, the symptoms are erased and progress very slowly. With adequate treatment, such patients live a long time, and death occurs from natural causes - due to age.
Statistics:
- At the beginning of 2014, there were 35 million people in the world diagnosed with HIV;
- The increase in people infected in 2013 was 2.1 million, deaths from AIDS - 1.5 million;
- The number of registered HIV carriers among the entire world population is approaching 1%;
- In the Russian Federation in 2013, there were 800 thousand infected and sick people, that is, about 0.6% of the population is affected by HIV;
- 90% of all AIDS cases in Europe occur in Ukraine (70%) and the Russian Federation (20%).

HIV prevalence by country (percentage of virus carriers among adults)
Data:
- HIV is more often detected in men than in women;
- In the last 5 years, cases of HIV detection in pregnant women have become more frequent;
- Residents of northern European countries become infected and suffer from AIDS much less often than southerners;
- Africans are most susceptible to the immunodeficiency virus, approximately 2/3 of all sick and infected people are in Africa;
- Those infected with the virus over the age of 35 develop AIDS 2 times faster than younger people.
Characteristics of the virus
HIV belongs to the group retroviruses HTLV group and family lentiviruses(“slow” viruses). It has the appearance of spherical particles, 60 times smaller in size than a red blood cell. It dies quickly in an acidic environment, under the influence of 70% ethanol, 3% hydrogen peroxide or 0.5% formaldehyde. Sensitive to heat treatment– becomes inactive after 10 minutes. already at +560°C, at 1000°C – within a minute. Resistant to ultraviolet radiation, radiation, freezing and drying.
Blood with HIV that gets on various objects remains infectious for up to 1-2 weeks.
HIV constantly changes its genome, each subsequent virus differs from the previous one by one step of the RNA - nucleotide chain. The HIV genome is 104 nucleotides long, and the number of errors during reproduction is such that after about 5 years nothing remains of the original combinations: HIV mutates completely. Consequently, previously used drugs become ineffective, and new ones have to be invented.

Although in nature there are not even two absolutely identical HIV genomes, some groups of viruses have typical signs. Based on them, all HIV are classified into groups, numbered 1 to 4.
- HIV-1: the most common, this group was the first to be discovered (1983).
- HIV-2: Less likely to be contracted than HIV-1. Those infected with type 2 do not have immunity to type 1 of the virus.
- HIV-3 and 4: rare variations, do not particularly affect the spread of HIV. In the formation of a pandemic (a general epidemic covering countries on different continents), HIV-1 and 2 are of primary importance, with HIV-2 being more common in West African countries.
Development of AIDS
Normally, the body is protected from the inside: the main role is played by cellular immunity, in particular lymphocytes. T lymphocytes produced by the thymus (thymus gland), according to their functional responsibilities they are divided into T-helpers, T-killers and T-suppressors. Helpers“recognize” tumor cells and cells damaged by viruses, and activate T-killers, which destroy atypical formations. Suppressor T cells regulate the direction of the immune response, preventing it from launching a reaction against its own healthy tissues.

A T-lymphocyte affected by a virus becomes atypical, the immune system reacts to it as a foreign formation and “sends” T-killers to help. They destroy the former T-helper, the capsids are released and take with them part of the lipid membrane of the lymphocyte, becoming unrecognizable to the immune system. Then the capsids disintegrate, and new virions are introduced inside other T helper cells.

Gradually, the number of helper cells decreases, and inside the human body, the “friend or foe” recognition system ceases to function. In addition to this, HIV activates the mechanism of mass apoptosis(programmed death) of all types of T-lymphocytes. The result is active inflammatory reactions to resident (normal, permanent) and conditionally pathogenic microflora, and at the same time an inadequate response of the immune system to truly dangerous fungi and tumor cells. Immunodeficiency syndrome develops, and characteristic symptoms of AIDS appear.
Clinical manifestations
Symptoms of HIV depend on the period and stage of the disease, as well as on the form in which the impact of the virus primarily manifests itself. Periods of HIV They are divided into incubation, when there are no antibodies to the virus in the blood, and clinical - antibodies are detected, the first signs of the disease appear. IN clinical differentiate stages HIV:
- Primary, including two forms– asymptomatic and acute infection without secondary manifestations, with concomitant diseases;
- Latent;
- AIDS with secondary diseases;
- Terminal stage.
I. Incubation period The time from HIV infection to the onset of symptoms is called the serologic window. Serum reactions to the immunodeficiency virus are negative: specific antibodies have not yet been detected. The average incubation duration is 12 weeks; the period can be reduced to 14 days with concomitant STDs, tuberculosis, general asthenia, or increased to 10-20 years. During the entire period the patient dangerous as a source of HIV infection.
II. Stage of primary manifestations of HIV characterized seroconversion– the appearance of specific antibodies, serological reactions become positive. The asymptomatic form is diagnosed only by a blood test. Acute HIV infection occurs 12 weeks after infection (50-90% of cases).
First signs manifested by fever, various types of rash, lymphadenitis, sore throat (pharyngitis). Possible intestinal upset - diarrhea and abdominal pain, enlarged liver and spleen. A typical laboratory sign: mononuclear lymphocytes, which are found in the blood at this stage of HIV.
Secondary diseases appear in 10-15% of cases against the background of a transient decrease in the number of T-helper lymphocytes. The severity of the diseases is average, they are treatable. The duration of the stage is on average 2-3 weeks, in most patients it becomes latent.
Forms acute HIV infections:

III. Latent stage of HIV, lasts up to 2-20 years or more. Immunodeficiency progresses slowly, HIV symptoms are expressed lymphadenitis– enlarged lymph nodes. They are elastic and painless, mobile, the skin retains its normal color. When diagnosing latent HIV infection, the number of enlarged nodes is taken into account - at least two, and their location - at least 2 groups not connected by a common lymph flow (with the exception of inguinal nodes). Lymph moves in the same direction as venous blood, from the periphery to the heart. If 2 lymph nodes are enlarged in the head and neck area, then this is not considered a sign of the latent stage of HIV. A combined increase in groups of nodes located in the upper and lower parts of the body, plus a progressive decrease in the number of T-lymphocytes (helper cells) testify in favor of HIV.
IV. Secondary diseases, with periods of progression and remission, depending on the severity of manifestations, it is divided into stages (4 A-B). Persistent immunodeficiency develops against the background of massive death of T-helper cells and depletion of lymphocyte populations. Manifestations - various visceral (internal) and skin manifestations, Kaposi's sarcoma.
V. Terminal stage irreversible changes are inherent, treatment is ineffective. The number of T helper cells (CD4 cells) falls below 0.05x109/l, patients die weeks or months from the onset of the stage. In drug addicts who have been using psychoactive substances for several years, CD4 levels may remain almost within normal limits, but severe infectious complications (abscesses, pneumonia, etc.) develop very quickly and lead to death.
Kaposi's sarcoma
Sarcoma ( angiosarcoma) Kaposi is a tumor arising from the connective tissue and affecting the skin, mucous membranes and internal organs. Triggered by the herpes virus HHV-8; more common in men infected with HIV. The epidemic type is one of the reliable signs of AIDS. Kaposi's sarcoma develops in stages: it begins with the appearance spots 1-5 mm in size, irregular in shape, bright bluish-red or brown in color, with a smooth surface. In AIDS, they are bright, localized on the tip of the nose, hands, mucous membranes and on the hard palate.
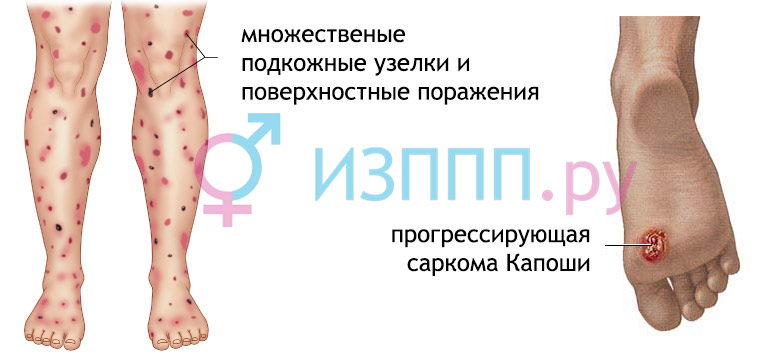
Then they are formed tubercles– papules, round or semicircular, up to 10 mm in diameter, elastic to the touch, can merge into plaques with a surface similar to an orange peel. Tubercles and plaques transform into nodular tumors 1-5 cm in size, which merge with each other and are covered ulcers. At this stage, sarcoma can be confused with syphilitic gummas. Syphilis is often combined with the immunodeficiency virus, like hepatitis C, shortening the incubation period and provoking the rapid development of acute symptoms of AIDS - lymphadenitis, damage to internal organs.
Kaposi's sarcoma is clinically divided into forms– acute, subacute and chronic. Each is characterized by the rate of tumor development, complications and prognosis regarding the duration of the disease. At acute form, the process quickly spreads, the cause of death is intoxication and extreme exhaustion ( cachexia), life time from 2 months to a maximum of 2 years. At subacute During the course of the disease, symptoms increase more slowly, life expectancy is 2-3 years; for the chronic form of sarcoma – 10 years, possibly more.
HIV in children
Incubation period lasts about a year if HIV was transmitted from mother to fetus. In case of infection through blood (parenteral) – up to 3.5 years; After transfusion of infected blood, the incubation is short, 2-4 weeks, and the symptoms are severe. HIV infection in children primarily affects the nervous system(up to 80% of cases); long-term, lasting up to 2-3 years, bacterial inflammation; with damage to the kidneys, liver and heart.
Very often develops Pneumocystis or lymphocytic pneumonia, inflammation of the parotid salivary glands ( mumps, he's a pig). HIV manifests itself at congenital dysmorphic syndrome– impaired development of organs and systems, in particular microcephaly – reduced size of the head and brain. A decrease in the blood level of gamma globulin fraction proteins is observed in half of those infected with HIV. Very rare Kaposi's sarcoma and hepatitis C, B.
Dysmorphic syndrome or HIV embryopathy determined in children infected with early timing of pregnancy. Manifestations: microcephaly, nose without membranes, the distance between the eyes is increased. The forehead is flat, the upper lip is split and protrudes forward. Strabismus, eyeballs protruding outward ( exophthalmos), the cornea is bluish in color. There is growth retardation, development does not correspond to norms. Prognosis for life in general negative, mortality is high during 4-9 months of life.

Manifestations of neuro-AIDS: chronic meningitis, encephalopathy(damage to brain tissue) with the development of dementia, damage to peripheral nerves with symmetrical disorders of sensitivity and trophism in the arms and legs. Children are significantly behind their peers in development, prone to convulsions and muscle hypertonicity, and may develop paralysis of the limbs. Diagnosis of HIV neuro-symptoms is based on clinical signs, blood tests and CT scan results. Layer-by-layer images reveal atrophy(reduction) of the cerebral cortex, expansion of the cerebral ventricles. HIV infection is characterized by calcium deposits in the basal ganglia of the brain. Progression of encephalopathy leads to death within 12-15 months.
Pneumocystis pneumonia: in children of the 1st year of life it is observed in 75% of cases, over a year - in 38%. Often, pneumonia develops by the age of six months; symptoms include high fever, rapid breathing, and a dry and persistent cough. Increased sweating, especially at night; weakness that only gets worse over time. Pneumonia is diagnosed after auscultation (according to the stages of development, weakened breathing is heard first, then small dry rales, in the resolution stage - crepitus, the sound is heard at the end of inspiration); X-ray (enhanced pattern, infiltration of pulmonary fields) and microscopy of biomaterial (pneumocystis are detected).
Lymphocytic interstitial pneumonia: a unique disease associated specifically with childhood AIDS; there are no concomitant infections. The partitions between the alveoli and the tissue around the bronchi become denser, where lymphocytes and other immune cells are found. Pneumonia begins unnoticed and develops slowly; among the initial symptoms, a long dry cough and dry mucous membranes are typical. Then shortness of breath appears and respiratory failure increases sharply. The X-ray image shows thickening of the lung fields, enlarged lymph nodes in the mediastinum - the space between the lungs.
Laboratory tests for HIV
The most common method for diagnosing HIV is (ELISA or ELISA test), which is used to detect the immunodeficiency virus. Antibodies to HIV are formed between three weeks and 3 months after infection and are detected in 95% of cases. After six months, HIV antibodies are found in 9% of patients, later - only in 0.5-1%.
As biomaterial use blood serum taken from a vein. You can get a false-positive ELISA result if HIV infection is accompanied by autoimmune (lupus, rheumatoid arthritis), cancer or chronic infectious diseases (tuberculosis, syphilis). A false negative response occurs during the so-called period. seronegative window, when antibodies have not yet appeared in the blood. In this case, to control HIV, you need to donate blood again, after a pause of 1 to 3 months.

If the ELISA is assessed as positive, the HIV test is duplicated using a polymerase chain reaction, determining the presence of viral RNA in the blood. The technique is highly sensitive and specific and does not depend on the presence of antibodies to the immunodeficiency virus. Immunoblotting is also used, which makes it possible to detect antibodies to HIV protein particles with precise molecular weights (41, 120 and 160 thousand). Their identification gives the right to make a final diagnosis without confirmation by additional methods.
HIV test Necessarily This is done only during pregnancy; in other cases, a similar examination is voluntary. Doctors do not have the right to disclose the diagnosis; all information about patients and people infected with HIV is confidential. Patients have the same rights as healthy people. Criminal punishment is provided for the deliberate spread of HIV (Article 122 of the Criminal Code of the Russian Federation).
Principles of treatment
HIV treatment is prescribed after a clinical examination and laboratory confirmation of the diagnosis. The patient is constantly monitored, repeated blood tests are carried out during antiviral therapy and after treatment of HIV manifestations.
A cure for HIV has not yet been invented, and there is no vaccine. It is impossible to remove the virus from the body, and this is a fact at this time. However, one should not lose hope: active antiretroviral therapy (HAART) can reliably slow down and even practically stop the development of HIV infection and its complications.
The life expectancy of patients receiving modern treatment is 38 years (for men) and 41 years (women). The exception is the combination of HIV and hepatitis C, when less than half of the patients reach the 5-year survival threshold.
HAART– a technique based on the use of several pharmaceuticals at once that affect various mechanisms of the development of HIV symptoms. Therapy combines several goals at once.
- Virological: block the reproduction of the virus in order to reduce the viral load (the number of HIV copies in 1 ml3 of blood plasma) and keep it at a low level.
- Immunological: Stabilize the immune system to raise T-lymphocyte levels and restore the body's defenses against infections.
- Clinical: to increase the full life span of those infected with HIV, to prevent the development of AIDS and its manifestations.
Virological treatment
The human immunodeficiency virus is treated with drugs that prevent it from attaching to a T-lymphocyte and penetrating inside - this is inhibitors(suppressors) penetration. A drug Celzentry.
The second group of drugs consists of viral protease inhibitors, which is responsible for the formation of full-fledged viruses. When it is inactivated, new viruses are formed, but they cannot infect new lymphocytes. Drugs Kaletra, Viracept, Reyataz and etc.

The third group is inhibitors of reverse transcriptase, an enzyme that helps reproduce viral RNA in the lymphocyte nucleus. Drugs Zinovudine, Didanosine.Combination medications against HIV are also used, which need to be taken only once a day - Trizivir, Combivir, Lamivudine, Abacavir.
With simultaneous exposure to drugs, the virus cannot enter the lymphocytes and “multiply”. Upon appointment tritherapy The ability of HIV to mutate and develop insensitivity to drugs is taken into account: even if the virus becomes immune to one drug, the remaining two will still work. Dosage calculated for each patient, taking into account the state of health and possible side effects. A separate regimen is used for pregnant women, and after using HAART, the frequency of HIV transmission from mother to child decreases from 20-35% to 1-1.2%.
It is important to take your medications at the same time for the rest of your life: if the schedule is violated or the course is interrupted, treatment completely loses its meaning. Viruses quickly change their genome, becoming immune ( resistant) to therapy, and form numerous resistant strains. With such a development of the disease, choosing antiviral treatment is very problematic, and sometimes simply impossible. Cases of the development of resistance are more often observed among HIV-infected drug addicts and alcoholics, for whom strict adherence to the treatment schedule is unrealistic.
The drugs are effective, but their prices are high. For example, the cost of one-year treatment with Fuzeon (a group of penetration inhibitors) reaches $25 thousand, and the monthly cost when using Trizivir ranges from $1000.
note, that farm. funds almost always have two names - according to the active substance and the commercial name of the drug, which was given to it by the manufacturer. The prescription must be written exactly according to active substance, indicating its quantity in a tablet (capsule, ampoule, etc.). Substances with identical effects are often presented under different names. commercial names and may vary significantly in price. The pharmacist’s job is to offer the patient several options to choose from and guide them regarding the cost. Generics- analogues of original developments, always cost much less than “branded” drugs.
Immunological and clinical treatment
 Using an immunostimulant drug Inosine pranobex, due to which the level of lymphocytes increases, the activity of certain fractions of leukocytes is stimulated. The antiviral effect indicated in the annotation does not apply to HIV. Indications, relevant for HIV-infected people: viral hepatitis C, B; immunodeficiency states; cytomegalovirus; herpes simplex virus type 1; mumps. Dosages: adults and children 3-4 times/day. at the rate of 50-100 mg/kg. Well 5-15 days, can be repeated many times, but only under the supervision of an infectious disease specialist. Contraindications: increased levels of uric acid in the blood ( hyperuricemia), kidney stones, systemic diseases, pregnancy and breastfeeding.
Using an immunostimulant drug Inosine pranobex, due to which the level of lymphocytes increases, the activity of certain fractions of leukocytes is stimulated. The antiviral effect indicated in the annotation does not apply to HIV. Indications, relevant for HIV-infected people: viral hepatitis C, B; immunodeficiency states; cytomegalovirus; herpes simplex virus type 1; mumps. Dosages: adults and children 3-4 times/day. at the rate of 50-100 mg/kg. Well 5-15 days, can be repeated many times, but only under the supervision of an infectious disease specialist. Contraindications: increased levels of uric acid in the blood ( hyperuricemia), kidney stones, systemic diseases, pregnancy and breastfeeding.
Interferon group drug Viferon has antiviral and immunomodulatory activity. In the case of HIV (or AIDS), it is used for Kaposi's sarcoma, mycoses and hairy cell leukemia. The effect of the drug is complex: interferon enhances the activity of T-helper cells and increases the production of lymphocytes, and blocks the proliferation of viruses in several ways. Additional components - vitamin C, E - protect cells, and the effectiveness of interferon increases 12-15 times (synergistic effect). Viferon can be taken in long courses, its activity does not decrease over time. In addition to HIV, indications include any viral infections, mycoses (including internal organs), hepatitis C, B or D. When administered rectally the drug is used twice a day for a course of 5-10 days; ointment is not used for HIV. Pregnant women are prescribed starting from the 14th week.

Treatment of pulmonary manifestations
The main early manifestation of HIV infection is inflammation of the lungs.to their caused by pneumocystis (Pneumocystis carina), single-celled organisms similar to fungi and protozoa at the same time. In patients with AIDS, untreated Pneumocystis pneumonia is fatal in 40% of cases, and correct and timely prescribed therapeutic regimens help reduce the mortality rate to 25%. With the development of a relapse, the prognosis worsens, repeated pneumonia is less sensitive to treatment, and mortality reaches 60%.
Treatment: basic drugs – Biseptol (Bactrim) or pentamidine. They act in different directions, but ultimately lead to the death of pneumocystis. Biseptol is taken orally, pentamidine is injected into the muscles or into a vein. The course is from 14 to 30 days; for AIDS, it is preferable to use pentamidine. The drugs are not prescribed together, because their toxic effect is enhanced without a noticeable increase in the therapeutic effect.
Low toxic drug DFMO (alpha-difluoromethylornithine) acts on pneumocystis and simultaneously blocks the reproduction of retroviruses, which include HIV, and also has a beneficial effect on lymphocytes. The course is 2 months, the daily dosage is calculated based on 6 g per 1 square meter. meter of body surface and divide it into 3 steps.
With adequate treatment of pneumonia, improvement is noticeable already on days 4-5 from the start of therapy; after a month, in a quarter of patients, pneumocystis are not detected at all.
Immunity to HIV
Statistics of confirmed HIV resistance: among Europeans, 1% are completely immune to the immunodeficiency virus, up to 15% are partially immune. In both cases, the mechanisms are unclear. Scientists associate this phenomenon with the bubonic plague epidemics in Europe in the 14th and 18th centuries (Scandinavia), when, perhaps, in some people early genetic mutations became established in heredity. There is also a group of so-called. “non-progressors”, who make up about 10% of those infected with HIV, in whom AIDS symptoms do not appear for a long time. In general, there is no immunity to HIV.

A person is immune to the HIV-1 serotype if his body produces the TRIM5a protein, which is able to “recognize” the viral capsid and block the replication of HIV. The CD317 protein can keep viruses on the surface of cells, preventing them from infecting healthy lymphocytes, and CAML makes it difficult for new viruses to be released into the blood. The beneficial activity of both proteins is disrupted by hepatitis C and simplex viruses, therefore, with these concomitant diseases, the risks of HIV infection are higher.
Prevention
The fight against the AIDS epidemic and its consequences has been declared by WHO:

HIV prevention among drug addicts means explaining the dangers of infection through injections, providing disposable syringes and exchanging used ones for sterile ones. The latest measures seem strange and are associated with the spread of drug addiction, but in this case it is easier to at least partially stop the routes of HIV infection than to wean a huge number of drug addicts.
An HIV first aid kit will be useful to everyone in everyday life, in the workplace - for doctors and rescuers, as well as people in contact with people infected with HIV. Medicines are accessible and basic, but their use really reduces the risk of infection with the immunodeficiency virus:
- Alcohol solution of iodine 5%;
- Ethanol 70%;
- Dressing supplies (pack of sterile gauze swabs, bandages, plaster) and scissors;
- Sterile distilled water – 500 ml;
- Crystals of potassium permanganate (potassium permanganate) or hydrogen peroxide 3%;
- Eye pipettes (sterile, in packaging or in a case);
- Specific medications are provided only for physicians working at blood collection stations and in hospital emergency departments.

Blood that got into on the skin from an HIV-infected person, you should immediately wash it off with soap and water, then treat it with a swab soaked in alcohol. For an injection or cut through gloves they need to be removed, the blood squeezed out, hydrogen peroxide applied to the wound; then blot the foam, cauterize the edges of the wound with iodine and, if necessary, apply a bandage. Hit in the eyes: Rinse first with water, then with potassium permanganate solution (faint pink). Oral cavity: rinse with poor pink potassium permanganate, then with 70% ethanol. After unprotected intercourse: if possible, shower, then treat (douching, washing) the genitals with a rich pink solution of potassium permanganate.
AIDS prevention will be more effective if every person becomes conscious of their health. It is much easier to use a condom during sexual intercourse and avoid unwanted acquaintances (prostitutes, drug addicts) than to undergo long and expensive treatment later. To understand the picture of the danger of HIV, just compare the statistics: per year from fever Ebola About 8,000 people died, and more than 1.5 million died from HIV! conclusions are obvious and disappointing - in the modern world, the immunodeficiency virus has become a real threat to all humanity.
Video: educational film about HIV
Video: AIDS in the program “Live Healthy!”
Read also...